Introduction
A poxvirus infection of the skin, molluscum contagiosum1 presents with discrete, firm, flesh-colored, umbilicated papules.
Epidemiology
Affects children and young adults.
Etiology
This usually self-limited infection is normally acquired innocently by children through direct skin-to-skin contact, but when seen in adults, it is usually acquired sexually. It is caused by the largest of the DNA poxviruses. There are four viral subtypes, I, II, III, IV; most infections are caused by Type I. The average latency period for the virus is 2 months.2
Symptoms and clinical features
Often these lesions are completely asymptomatic but they can be mildly itchy. They start few in number and then spread. In a patient with HIV, they can be very extensive.
The discrete little dome-shaped, umbilicated, skin-colored papules can be scattered or in groups. They are usually found in the suprapubic area or inner thighs but may also be found on the buttocks or lower abdomen as well as the groin.
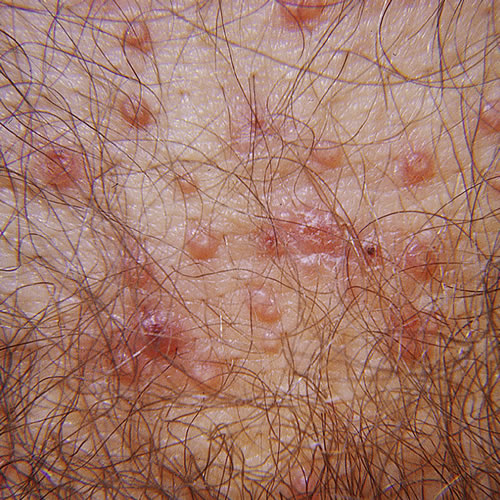
They may be pink or pearly in color and may have a waxy appearance. The central umbilication contains a white cord-like core and the lesions measure 1-3 mm (sometimes larger) in diameter.3
Diagnosis
Diagnosis is usually made clinically. The small umbilications and the smooth skin of the papules are characteristic. In late stages, there may be erythema around the lesions whereas normal surrounding skin is seen in earlier stages of infection.
Pathology/Laboratory Findings
Direct examination with Giemsa stain of material extruded from lesions shows the typical molluscum bodies. Cytoplasmic inclusion bodies within keratinocytes that contain large numbers of mature virions are characteristic on histological exam whereas the papules consist of acanthotic epithelium with hyperkeratosis.4
Differential diagnosis
Differential diagnosis includes warts, basal-cell carcinoma, and, in the immunocompromised, the deep fungi Cryptococcus neoformans and Histoplasma capsulatum
Treatment/management
Patients who are immunocompetent may have spontaneous resolution within three months if not treated.
Molluscum treatment involves destructive techniques:
- Liquid nitrogen is mainstay of therapy, every 1 to 2 weeks. Each lesion is individually treated with a white frosted 1 mm border. The liquid nitrogen is applied for 6-10 seconds. Pain associated with the procedure can be a problem, as can scarring afterward, including hypopigmentation in those with dark skin. The procedure is well tolerated by adults but may not be by children.
Alternatives include the following:
- Topical cantharidin 0.7% (Cantharone, a blistering agent that must be compounded) is applied in a thin film to the lesions and dried. The lesions are taped for two to four hours, and then washed off. This is repeated as needed every 2 to 3 weeks. Using one drop can make a nasty blister. Erythema, burning pain, and pruritus may occur after treatment although the liquid is painless when first applied. Scarring may also occur.
- Curettage with or without local anesthesia: In children, consider the use of lidocaine-prilocaine (EMLA) cream under occlusion for 1 to 1 1⁄2 hours before treatment.
- Light electrodesiccation with or without local anesthesia.
- Topical imiquimod cream is applied overnight for 3 non-consecutive nights a week for 12 weeks.5
- Podophyllotoxin; Podofilox 0.5% in a solution, gel or cream applied twice a day on three consecutive days in a week for up to four weeks. Safety in children is not established. Erythema, burning pain and pruritus may occur after treatment.
Immunocompromised individuals do well with anti-viral therapy, but if not treated, may not be able to become free of self-seeding infection.
References
- Fisher BK, Margesson, LJ. Genital Skin Disorders: Diagnosis and Treatment. Mosby, Inc., 1998. 135
- Lynch P. in Skin-Colored Lesions. In Edwards L and Lynch P. Genital Dermatology Atlas, 2nd edition. Wolters Kluwer/Lippincott Williams & Wilkins, 2011. 204.
- Heller DS, Wallach RC (.ed.) Vulvar Disease: a Clinicopathological Approach. Informa Healthcare USA, Inc., 2007. 75.
- Heller DS, Wallach RC (.ed.) Vulvar Disease: a Clinicopathological Approach. Informa Healthcare USA, Inc., 2007. 75.
- Theos AU, Cummins R, Silverberg NB, Paller AS. Effectiveness of imiquimod cream 55 for treating childhood molluscum contagiosum in a double-blind, randomized pilot trial. Cutis.2004; 74:134-138, 141-142.