Introduction
A furuncle1 is an abscess: a deep bacterial infection of hair follicles, forming a walled-off collection of pus in a painful, firm, or fluctuant mass. They are usually between 2 and 4 cm in size. A synonym for furuncle is boil. Coalescing abscesses form a carbuncle.
Epidemiology
Abscesses are most common in adolescents and young adults and more common in males than in females.
Etiology
Staphylococcus aureus and much less commonly, Escherichia coli or Pseudomonas aeruginosa are the cause of abscesses (furuncles.) The problem is found most commonly in those who are chronic carriers of Staphlococcus in the nares or perineum, and their infections are typically around areas of friction. Although more frequently present under the abdominal pannus in the obese, an abscess may appear in the vulvar area or the inner thigh or buttock.
Methicillin-resistant Staph aureus (MRSA) is becoming more wide spread as an etiological factor for abscesses. In the case of MRSA, the organism is resistant to any of the beta-lactam antibiotics: penicillins and cephalosporins. Staph aureus organisms which are sensitive to these antibiotics are labeled MSSA. (MRSA document).
Symptoms and clinical features
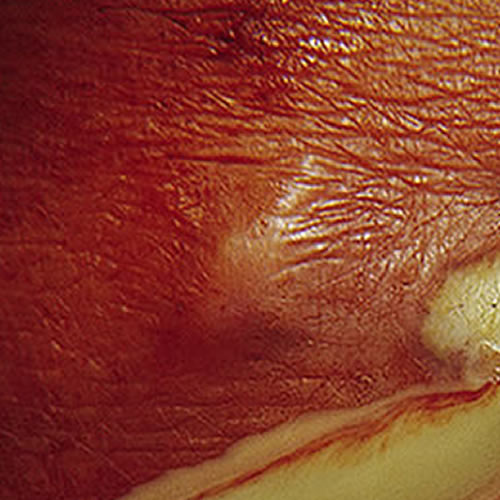
An exquisitely tender localized lesion forms, throbbing with pain, sometimes accompanied by malaise and a low-grade fever. In the groin, inner thighs, or perianal area, a hard, red nodule develops that may progress to a fluctuant mass with a central necrotic plug. The surface may show exuding pus.

Diagnosis
The clinical picture, plus the culture, determines the diagnosis.
Pathology/Laboratory Findings
Culture of the purulent drainage determines the diagnosis, with Gram stain of the drainage confirming the organisms. Biopsy is usually not necessary. In small lesions, culture is not necessary and may be difficult to obtain without incision.
Differential diagnosis
Differential diagnosis includes hidradenitis suppurativa, severe herpes simplex, and ruptured epidermal cyst.
Treatment/management
With a simple lesion, local application of heat and drainage may be all that is necessary, along with the usual recommendations for loose, non-binding clothing, warm soaks, patting dry, etc. Deeper lesions may need packing after drainage.
Antibiotics are used for severe or recurrent disease. See table below. The choice depends on the culture and sensitivity. For Staphlococcus aureus, Cloxacillin 500 mg orally 4 x a day, Cephalexin 250 mg orally 4 x a day, Erythromycin 250 mg orally 4 x a day are prescribed (adjust doses depending on the patient’s size). The possibility of Methicillin-resistant S.Aureus infection must be kept in mind. Reasonable antibiotics for treatment of MRSA include Clindamycin (300 to 450 mg every six to eight hours), Trimethoprim-sulfamethoxazole (two double-strength tablets twice daily), and long-acting tetracycline (such as doxycycline or minocycline) 100 mg twice daily. Treatment length varies with the severity of the infection.
For those with nasal or gluteal cleft carriage, use Mupirocin (Bactroban) or Fusidic Acid (Fucidin) ointment applied 4 times a day for one week.
For continued recurrences, a combination of Cloxacillin and Rifampin is used.