Introduction
An epidermal cyst1, the most common cutaneous cyst, is also the most common genital cyst in women. It consists of the subcutaneous enclosure by a layer of stratified squamous epithelium of keratin and lipid-rich debris. The sac can rupture, causing pain. These occur most commonly in the labia majora and minora, not in the vestibule.
Synonyms for epidermal cysts are keratinous cyst, epidermal inclusion cyst, sebaceous cyst, wen, infundibular cyst, and epidermoid cyst.
Epidemiology
These are common, although the exact prevalence is unknown. They occur most often in mid-life2 but may occur at any age.
Etiology
There is entrapment of epidermal cells in the dermis, sometimes secondary to trauma, or, more commonly, there is blockage of the pilosebaceous duct resulting in distention and cyst formation. These are single or multiple asymptomatic nodules within the vulvar skin. Their size is variable. The very tiny (1-2 mm) cysts are known as milia.
Symptoms and clinical features
Patients may be unaware of the presence of simple cysts as they are usually asymptomatic, but some become worried about finding unexplained lumps.
If the cyst is traumatized, the patient complains of pain and tenderness. If the cyst ruptures, the patient complains of an unpleasant, cheesy odor. There may be so many cysts that any pressure in the area can be quite uncomfortable.
Single cysts are typically round, firm, and smooth, mobile, subcutaneous nodules and may have a barely visible, keratin-filled orifice. These dermal nodules range in size from 2 to 3 mm up to 1 to 2 cm and are located along the labia majora and, less commonly, the labia minora. They can be multiple, sometimes forming a cobblestone effect. The skin surface is smooth, and the skin is a yellowish color.

There may be an obvious comedonal plug at the opening.
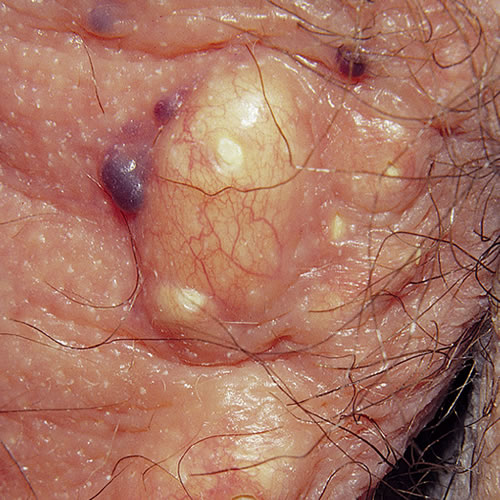
With pressure or with a minor incision, yellow or cream-colored, smelly, cheesy material can be expressed. If there has been trauma and rupture of the cyst, it may be erythematous and tender like a furuncle.
Diagnosis
Diagnosis is clinical and can be confirmed on biopsy.
Pathology/laboratory findings
Biopsy if the diagnosis is unclear.
Differential diagnosis
Neuroma, dermal nevus, xanthoma, furuncle, molluscum contagiosum and hidradenitis suppurativa.
Treatment
Asymptomatic, indolent, vulvar cysts need no treatment. Reassure the patient that the cysts are harmless.
Symptomatic cysts are surgically removed under local anesthesia.
Inflamed cysts should not be excised. They may be infected or simply ruptured with foreign body reaction. They should be treated with a tetracycline antibiotic (partly as an anti-inflammatory) and, if there is true infection with abscess formation, drainage should be carried out first.
Recurrent inflamed cysts benefit from long-term anti-inflammatory antibiotics:
Tetracycline or Erythromycin 500 mg orally twice a day
OR
Doxycycline or Minocycline 100 mg orally twice a day
OR
Clindamycin 150 mg orally twice a day
OR
Double strength trimethoprim-sulfamethoxazole orally twice a day.3
References
- Fisher BK, Margesson, LJ. Genital Skin Disorders: Diagnosis and Treatment. Mosby, Inc., 1998. 202-203.
- Neil S. White lesions. In Edwards L and Lynch PJ. Genital Dermatology Atlas, 2nd ed. Wolters Kluwer/Lippincott Williams & Wilkins. Philidelphia. 2011. 194.
- Edwards L. Yellow and pustular lesions. In Edwards L and Lynch PJ. Genital Dermatology Atlas, 2nd ed. Wolters Kluwer/Lippincott Williams & Wilkins. Philidelphia. 2011. 118.